Dangers of Koi Pah & Vitamin Toxicity
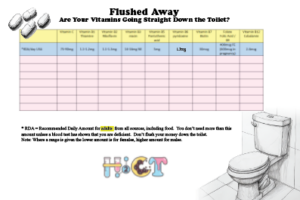
Print the sheet below to check your vitamin intake from supplements compared to the RDA:
Write down the amount of each vitamin that is in the vitamin tablets that you take.
Fat Soluble Vitamins A, D, E and K
Fat soluble Vitamins A, D, E and K are stored in the body, please do not take fat soluble vitamins without a blood test to show that you are deficient. Listen to your doctors advice and get follow up blood tests.
Water Soluble Vitamins
The information below is about the upper limits for water soluble vitamins. This is the amount beyond which your body cannot eliminate it all without negative consequences on your health. It is not necessary to take more that the recommended daily amount (RDA), unless you are deficient. Excess up to the upper limit will be excreted in the urine, so it is a waste of your money. But if you still want to take more than the RDA, then check that you are not ingesting above the tolerable upper limits.
More information on each vitamin including it’s food sources and functions can be found at https://ods.od.nih.gov/factsheets
Health Risks from Excessive Thiamine B1
Recommended Daily Intake for adults = 75-90mg
The body excretes excess amounts of thiamin in the urine. Because of the lack of reports of adverse effects from high thiamin intakes (50 mg/day or more) from food or supplements, the FNB did not establish ULs for thiamin. They hypothesize that the apparent lack of toxicity may be explained by the rapid decline in absorption of thiamin at intakes above 5 mg. However, the FNB noted that in spite of the lack of reported adverse events, excessive intakes of thiamin could have adverse effects.
Health Risks from Excessive Riboflavin B2
Recommended Daily Intake for adults = 1.1-1.3mg
Intakes of riboflavin from food that are many times the RDA have no observable toxicity, possibly because riboflavin’s solubility and capacity to be absorbed in the gastrointestinal tract are limited. Because adverse effects from high riboflavin intakes from foods or supplements (400 mg/day for at least 3 months) have not been reported, the FNB did not establish ULs for riboflavin. The limited data available on riboflavin’s adverse effects do not mean, however, that high intakes have no adverse effects, and the FNB urges people to be cautious about consuming excessive amounts of riboflavin.
Health Risks from Excessive Niacin B3
Recommended Daily Intake for adults = 14-16mg
No adverse effects have been reported from the consumption of naturally occurring niacin in foods. However, high intakes of both nicotinic acid and nicotinamide taken as a dietary supplement or medication can cause adverse effects, although their toxicity profiles are not the same.
Thirty to 50 mg or more nicotinic acid typically causes flushing; the skin on the patient’s face, arms, and chest turns a reddish color because of vasodilation of small subcutaneous blood vessels. The flushing is accompanied by burning, tingling, and itching sensations. These signs and symptoms are typically transient and can occur within 30 minutes of intake or over days or weeks with repeated dosing; they are considered an unpleasant, rather than a toxic, side effect. However, the flushing can be accompanied by more serious signs and symptoms, such as headache, rash, dizziness, and/or a decrease in blood pressure. Supplement users can reduce the flushing effects by taking nicotinic acid supplements with food, slowly increasing the dose over time, or simply waiting for the body to develop a natural tolerance.
When taken in pharmacologic doses of 1,000 to 3,000 mg/day, nicotinic acid can also cause more serious adverse effects. Many of these effects have occurred in patients taking high-dose nicotinic acid supplements to treat hyperlipidemias. These adverse effects can include hypotension severe enough to increase the risk of falls; fatigue; impaired glucose tolerance and insulin resistance; gastrointestinal effects, such as nausea, heartburn, and abdominal pain; and ocular effects, such as blurred or impaired vision and macular edema (a buildup of fluid at the center of the retina). High doses of nicotinic acid taken over months or years can also be hepatotoxic; effects can include increased levels of liver enzymes; hepatic dysfunction resulting in fatigue, nausea, and anorexia; hepatitis; and acute liver failure. Hepatotoxicity is more likely to occur with the use of extended-release forms of nicotinic acid .
To minimize the risk of adverse effects from nicotinic acid supplementation or to identify them before they become serious, the American College of Cardiology and the American Heart Association recommend measuring hepatic transaminase, fasting blood glucose or hemoglobin A1C (33.8 degrees Fahrenheit), and uric acid levels in all supplement users before they start therapy, while the dose is being increased to a maintenance level, and every 6 months thereafter. The societies also recommend that patients not use nicotinic acid supplements or stop using them if their hepatic transaminase levels are more than two or three times the upper limits of normal; if they develop persistent hyperglycemia, acute gout, unexplained abdominal pain, gastrointestinal symptoms, new-onset atrial fibrillation, or weight loss; or if they have persistent and severe skin reactions, such as flushing or rashes.
Nicotinamide does not cause skin flushing and has fewer adverse effects than nicotinic acid, and these effects typically begin with much higher doses. Nausea, vomiting, and signs of liver toxicity can occur with nicotinamide intakes of 3,000 mg/day. In several small studies of participants undergoing hemodialysis, the most common adverse effects from 500–1,500 mg/day nicotinamide supplementation for several months were diarrhea and thrombocytopenia (low platelet count).
The FNB has established ULs for niacin that apply only to supplemental niacin for healthy infants, children, and adults. These ULs are based on the levels associated with skin flushing. The FNB acknowledges that although excess nicotinamide does not cause flushing, a UL for nicotinic acid based on flushing can prevent the potential adverse effects of nicotinamide. The UL, therefore, applies to both forms of supplemental niacin. However, the UL does not apply to individuals who are receiving supplemental niacin under medical supervision.
Tolerable Upper Intake Levels (ULs) for Niacin
| Age | Male | Female | Pregnancy | Lactation |
| 0–12 months | Not possible to establish* | Not possible to establish* | ||
| 1–3 years | 10 mg | 10 mg | ||
| 4–8 years | 15 mg | 15 mg | ||
| 9–13 years | 20 mg | 20 mg | ||
| 14–18 years | 30 mg | 30 mg | 30 mg | 30 mg |
| 19+ years | 35 mg | 35 mg | 35 mg | 35 mg |
*Breast milk, formula, and food should be the only sources of niacin for infants.
Health Risks from Excessive Pantothenic Acid B5
Recommended Daily Intake = 5mg
The FNB was unable to establish ULs for pantothenic acid because there are no reports of pantothenic acid toxicity in humans at high intakes. Some individuals taking large doses of pantothenic acid supplements (e.g., 10 g (0.35 ounces)/day) develop mild diarrhea and gastrointestinal distress, but the mechanism for this effect is not known.
Health Risks from Excessive Vitamin B6
Recommended Daily Intake for adults = 1.3mg
High intakes of vitamin B6 from food sources have not been reported to cause adverse effects. However, chronic administration of 1–6 g (0.21 ounces) oral pyridoxine per day for 12–40 months can cause severe and progressive sensory neuropathy characterized by ataxia (loss of control of bodily movements). Symptom severity appears to be dose dependent, and the symptoms usually stop if the patient discontinues the pyridoxine supplements as soon as the neurologic symptoms appear. Other effects of excessive vitamin B6 intakes include painful, disfiguring dermatological lesions; photosensitivity; and gastrointestinal symptoms, such as nausea and heartburn.
The scientific literature includes isolated case reports of congenital defects in the infants of individuals who took pyridoxine supplements during the first half of pregnancy. However, a more recent observational study found no association between pyridoxine supplementation (mean dose 132.3 ± 74 mg/day) in pregnant people starting at 7 weeks gestation and continuing for 9 ± 4.2 weeks and teratogenic effects in their infants.
The FNB has established ULs for vitamin B6 that apply to both food and supplement intakes (Table 3). The FNB noted that although several reports show sensory neuropathy occurring at doses lower than 500 mg/day, studies in patients treated with vitamin B6 (average dose of 200 mg/day) for up to 5 years found no evidence of this effect. Based on limitations in the data on potential harms from long-term use, the FNB halved the dose used in these studies to establish a UL of 100 mg/day for adults. ULs are lower for children and adolescents based on body size. The ULs do not apply to individuals receiving vitamin B6 for medical treatment, but such individuals should be under the care of a physician.
Tolerable Upper Intake Levels (ULs) for Vitamin B6
| Age | Male | Female | Pregnancy | Lactation |
| 0–12 months | Not possible to establish* | Not possible to establish* | ||
| 1–3 years | 30 mg | 30 mg | ||
| 4–8 years | 40 mg | 40 mg | ||
| 9–13 years | 60 mg | 60 mg | ||
| 14–18 years | 80 mg | 80 mg | 80 mg | 80 mg |
| 19+ years | 100 mg | 100 mg | 100 mg | 100 mg |
*Breast milk, formula, and food should be the only sources of vitamin B6 for infants.
In 2023, the Panel on Nutrition, Novel Foods and Food Allergens of the European Food Safety Authority (EFSA) released a scientific opinion on the tolerable upper intake levels for vitamin B6. Based on systematic reviews that examined associations between vitamin B6 and peripheral neuropathy, the panel set an upper limit for vitamin B6 of 12 mg/day for all adults, including those who are pregnant or lactating, with lower amounts ranging from 2.2 to 10.7 mg/day for infants and children, depending on age.
Health Risks from Excessive Biotin B7
Recommended Daily Intake for adults = 30mcg
The FNB was unable to establish ULs for biotin because there is no evidence in humans that biotin is toxic at high intakes. Several studies have found no adverse effects of 10–50 mg/day biotin, and up to 200 mg/day oral biotin or 20 mg/day intravenously in patients with biotinidase deficiency do not produce symptoms of toxicity.
High biotin intakes, and potentially even intakes greater than the AI, may pose another type of health risk. Supplementing with biotin beyond recommended intakes can cause clinically significant falsely high or falsely low laboratory test results, depending on the test. These incorrect results may lead to inappropriate patient management or misdiagnosis of a medical condition. The following section has more details on these interactions.
Very high intakes of biotin may interfere with diagnostic assays that use biotin-streptavidin technology and are commonly used to measure levels of hormones (such as thyroid hormone) and other analytes such as 25-hydroxyvitamin D, producing falsely normal or abnormal results. As a result, a few recent case reports have described findings falsely indicating Graves’ disease and severe hyperthyroidism in patients taking 10–300 mg biotin per day, including six children receiving high doses of biotin (2–15 mg/kg body weight per day) to treat inherited metabolic diseases.
Even a single 10 mg dose of biotin has interfered with thyroid function tests administered within 24 hours of taking the supplement. A small study in six healthy adults who took 10 mg/day of supplemental biotin for 1 week found interference in several biotinylated assays, including falsely decreased levels of thyroid stimulating hormone (which could lead to a misdiagnosis of thyrotoxicosis) and N-terminal pro-brain natriuretic peptide (which could result in a failure to identify congestive heart failure). According to FDA, a patient with a high intake of supplemental biotin died following a troponin test (to help diagnose a heart attack) that gave a falsely low result because the test was subject to biotin interference.
FDA advises health care providers to ask their patients about any supplements they may be taking that contain biotin and to consider biotin interference as a possible source of error if laboratory test results do not match the clinical presentation of the patient.
Health Risks from Excessive Folate
Recommended Daily Intake for adults = 400mcg, 600mcg in pregnancy
Large amounts of folate can correct the megaloblastic anemia, but not the neurological damage, that can result from vitamin B12 deficiency. Some experts have therefore been concerned that high intakes of folate supplements might mask vitamin B12 deficiency until its neurological consequences become irreversible. Questions about this possibility still remain, but the focus of concern has shifted to the potential for large amounts of folate to precipitate or exacerbate the anemia and cognitive symptoms associated with vitamin B12 deficiency.
Concerns have also been raised that high folic acid intakes might accelerate the progression of preneoplastic lesions, increasing the risk of colorectal and possibly other cancers in certain individuals. In addition, intakes of 1,000 mcg per day or more of folic acid from supplements during the periconception period have been associated with lower scores on several tests of cognitive development in children at age 4–5 years than in children of mothers who took 400 mcg to 999 mcg.
Intakes of folic acid that exceed the body’s ability to reduce it to THF lead to unmetabolized folic acid in the body, which has been linked to reduced numbers and activity of natural killer cells, suggesting that it could affect the immune system. In addition, some scientists have hypothesized that unmetabolized folic acid might be related to cognitive impairment among older adults. These potential negative health consequences are not well understood and warrant further research.
Studies have found unmetabolized folic acid in blood from children, adolescents, and adults; breastmilk; and cord blood from newborns. Limited research suggests that single doses of 300 mcg or 400 mcg folic acid (a common amount in folic acid-containing supplements or servings of fortified foods, such as breakfast cereals) result in detectable serum levels of unmetabolized folic acid, whereas doses of 100 mcg or 200 mcg do not. In addition, a dose-frequency interaction appears to occur in which smaller amounts of folic acid consumed more frequently produce higher unmetabolized folic acid concentrations than the same total dose consumed in larger, less frequent amounts.
Based on the metabolic interactions between folate and vitamin B12, the FNB established a UL for the synthetic forms of folate available in dietary supplements and fortified foods (Table 3). The FNB did not establish a UL for folate from food because high intakes of folate from food sources have not been reported to cause adverse effects. Thus, unlike the RDAs, the ULs are in mcg, not mcg DFE. For folic acid, 1,000 mcg is equivalent to 1,667 mcg DFE because 0.6 mcg folic acid = 1 mcg DFE. The ULs do not apply to individuals taking high doses of supplemental folate under medical supervision.
Tolerable Upper Intake Levels (ULs) for Folate from Supplements or Fortified Foods
| Age | Male | Female | Pregnancy | Lactation |
| Birth to 12 months | Not possible to establish* | Not possible to establish* | ||
| 1–3 years | 300 mcg | 300 mcg | 300 mcg | 300 mcg |
| 4–8 years | 400 mcg | 400 mcg | 400 mcg | 400 mcg |
| 9–13 years | 600 mcg | 600 mcg | 600 mcg | 600 mcg |
| 14–18 years | 800 mcg | 800 mcg | 800 mcg | 800 mcg |
| 19+ years | 1,000 mcg | 1,000 mcg | 1,000 mcg | 1,000 mcg |
* Breast milk, formula, and food should be the only sources of folate for infants.
Health Risks from Excessive Vitamin B12
The FNB did not establish a UL for vitamin B12 because of its low potential for toxicity. Even at large doses, vitamin B12 is generally considered to be safe because the body does not store excess amounts.
Health Risks from Excessive Vitamin C
Vitamin C has low toxicity and is not believed to cause serious adverse effects at high intakes. The most common complaints are diarrhea, nausea, abdominal cramps, and other gastrointestinal disturbances due to the osmotic effect of unabsorbed vitamin C in the gastrointestinal tract.
In postmenopausal women with diabetes who participated in the Iowa Women’s Health Study, supplemental (but not dietary) vitamin C intake (at least 300 mg/day) was significantly associated with an increased risk of cardiovascular disease mortality. The mechanism for this effect, if real, is not clear and this finding is from a subgroup of patients in an epidemiological study. No such association has been observed in any other epidemiological study, so the significance of this finding is uncertain. High vitamin C intakes also have the potential to increase urinary oxalate and uric acid excretion, which could contribute to the formation of kidney stones, especially in individuals with renal disorders. However, studies evaluating the effects on urinary oxalate excretion of vitamin C intakes ranging from 30 mg to 10 g (0.35 ounces)/day have had conflicting results, so it is not clear whether vitamin C actually plays a role in the development of kidney stones. The best evidence that vitamin C contributes to kidney stone formation is in patients with pre-existing hyperoxaluria.
Due to the enhancement of nonheme iron absorption by vitamin C, a theoretical concern is that high vitamin C intakes might cause excess iron absorption. In healthy individuals, this does not appear to be a concern. However, in individuals with hereditary hemochromatosis, chronic consumption of high doses of vitamin C could exacerbate iron overload and result in tissue damage.
Under certain conditions, vitamin C can act as a pro-oxidant, potentially contributing to oxidative damage. A few studies in vitro have suggested that by acting as a pro-oxidant, supplemental oral vitamin C could cause chromosomal and/or DNA damage and possibly contribute to the development of cancer. However, other studies have not shown increased oxidative damage or increased cancer risk with high intakes of vitamin C.
Other reported effects of high intakes of vitamin C include reduced vitamin B12 and copper levels, accelerated metabolism or excretion of ascorbic acid, erosion of dental enamel, and allergic responses. However, at least some of these conclusions were a consequence of assay artifact, and additional studies have not confirmed these observations.
The FNB has established ULs for vitamin C that apply to both food and supplement intakes (Table 3). Long-term intakes of vitamin C above the UL may increase the risk of adverse health effects. The ULs do not apply to individuals receiving vitamin C for medical treatment, but such individuals should be under the care of a physician.
Tolerable Upper Intake Levels (ULs) for Vitamin C
| Age | Male | Female | Pregnancy | Lactation |
| 0–12 months | Not possible to establish* | Not possible to establish* | ||
| 1–3 years | 400 mg | 400 mg | ||
| 4–8 years | 650 mg | 650 mg | ||
| 9–13 years | 1,200 mg | 1,200 mg | ||
| 14–18 years | 1,800 mg | 1,800 mg | 1,800 mg | 1,800 mg |
| 19+ years | 2,000 mg | 2,000 mg | 2,000 mg | 2,000 mg |
*Formula and food should be the only sources of vitamin C for infants.
My Cookbook
 Stores that sell my book listed by country:
http://bit.ly/ARcookbook
All recipe quantities in the book are in grams, ounces and cups.
Stores that sell my book listed by country:
http://bit.ly/ARcookbook
All recipe quantities in the book are in grams, ounces and cups.











Thank you SO MUCH for this, Anne! You’ve saved me from inadvertently causing myself harm with the vitamin thing. I never used to take ANY supplements, however a few years ago a blood test showed I needed supplementing with folate, the doctor prescribed some and left me to it. But then the prescription ran out and it was too much hassle to try to jump through hoops to get it re-done, so finding folate supplements online, instead I just bought it myself instead of getting it on prescription. I was also advised by my doctor to supplement calcium after hysterectomy, so I also bought a calcium supplement myself online.
And while YES, I’ve been supplementing *on the advice of a doctor* I STILL managed to mess up! Because while the folate-only supplement I was originally prescribed was probably fine, I couldn’t find folate ONLY online, so it came with other B vitamins included as well. Same with the calcium – it also comes with vitamin D, zinc, magnesium etc.
So for the past couple of years I’ve been taking these THINKING I was doing what the doctor ordered, without ACTUALLY looking properly at the AMOUNTS on the packet.
And honestly, the folate one is going straight in the bin because one of the values turns out to be over 1,000% of the recommended intake – the others are 300%, 700% etc – only ONE of the vitamins reads as “100%” of the recommended amount!
The calcium supplement is at least better – all of those values are below 100%, so those can stay, but YIKES, I’m glad you told me before anything noticable happened. Lesson learned and THANK YOU again!